
The Outer Ear and the Inner Ear Are Not the Same Thing
Hearing is typically among the first questions families ask after a microtia diagnosis. The ear’s external structure and its internal hearing function are often assumed to be related — but understanding how microtia affects each requires separating them.
The clinical answer is more nuanced than a simple yes or no — and understanding the distinction has practical implications for early intervention.
This is the single most important concept for families to understand early. The human ear has three distinct parts — the outer ear, the middle ear, and the inner ear — and they develop through different biological processes during pregnancy.
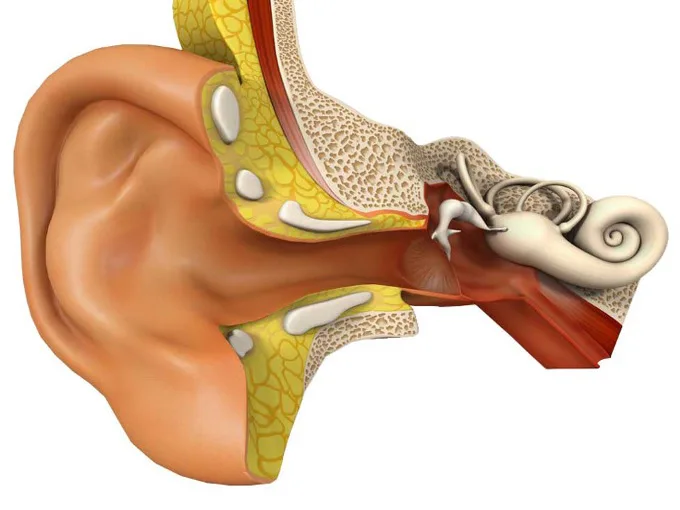
Microtia affects the outer ear. It is a condition of the auricle — the visible structure on the side of the head — and in many cases it also affects the ear canal, a condition called aural atresia. What microtia does not typically affect is the inner ear, where the cochlea and auditory nerve live. These structures develop from different embryological tissue and on a different timeline.
This distinction matters enormously. The cochlea is responsible for converting sound vibrations into the electrical signals the brain interprets as sound. In the overwhelming majority of children with microtia — including severe Grade III cases — the cochlea and auditory nerve are completely normal and fully intact.
In the overwhelming majority of children with microtia — the cochlea and auditory nerve are completely normal and fully intact.
So Why Is There Hearing Loss?
If the inner ear is typically normal, why do so many children with microtia have reduced hearing on the affected side?
The answer lies in the middle ear and the ear canal. Sound normally travels through the ear canal, vibrates the eardrum, and is conducted through three tiny bones in the middle ear — the malleus, incus, and stapes — before reaching the cochlea. In children with microtia and aural atresia, this pathway is interrupted. There is no open canal for sound to travel through, and the middle ear bones may be underdeveloped or malformed.
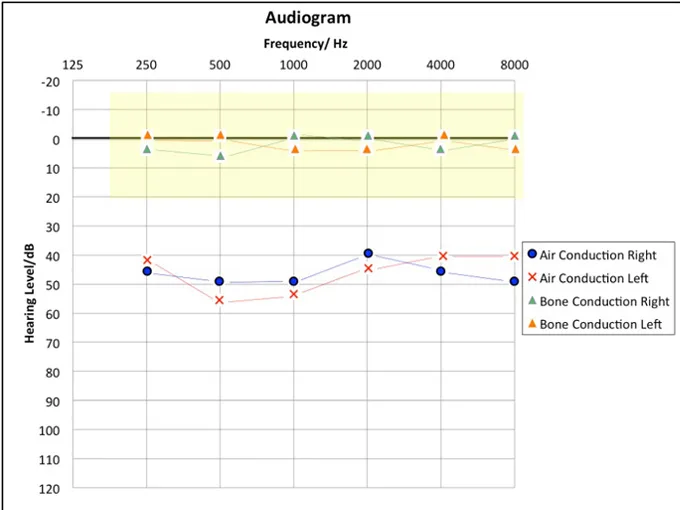
This type of hearing loss is called conductive hearing loss. It is a mechanical problem — a blockage in the pathway — rather than a problem with the hearing nerve itself. And because the nerve is intact, conductive hearing loss is generally very manageable with the right intervention.
What This Means for Your Child
A child with unilateral microtia — meaning one ear is affected — has one completely normal ear doing the full work of hearing. Most children in this situation develop speech and language on a completely typical timeline. They attend regular school, participate in all normal activities, and navigate the world without significant limitation.
That said, there are real considerations. Hearing in one ear makes it harder to localize sound — to identify which direction a sound is coming from. In noisy environments like classrooms, children with unilateral hearing loss sometimes struggle more than their peers to filter out background noise and focus on a single voice. These challenges are real and worth taking seriously, even when they are manageable.
For children with bilateral microtia — both ears affected — hearing intervention becomes more urgent. When both ears have conductive hearing loss, the impact on speech and language development is more significant. For children with bilateral microtia, early hearing support is not optional — it is clinically essential for language development.
For children with bilateral microtia, early hearing support is not optional — it is clinically essential for language development.
The First Step: A Formal Hearing Evaluation
Regardless of the grade of microtia or whether one or both ears are affected, a formal hearing evaluation should happen as early as possible — ideally within the first two months of life.
The standard test for newborns and infants is called an Auditory Brainstem Response test, or ABR. It measures how the auditory nerve and brain responds to sound and can be performed while an infant is sleeping. It does not require any cooperation from the child and provides highly reliable information about the function of the inner ear and hearing nerve.
The results of an ABR test do several things at once. They confirm whether the inner ear is functioning normally. They establish a baseline for monitoring. And they provide the foundation for any hearing intervention decisions — whether that means a bone conduction hearing device, monitoring, or something else entirely.
Hearing Devices for Microtia Patients
For children with aural atresia, the most common early hearing solution is a bone conduction hearing device worn on a soft headband. Unlike conventional hearing aids, which amplify sound through the ear canal, bone conduction devices transmit sound vibrations directly through the skull to the cochlea — bypassing the blocked canal entirely.
These devices are safe, non-invasive, and remarkably effective. For many children they make a meaningful difference in sound clarity and background noise management from a very early age. For children with bilateral microtia they are not a preference — they are a priority.
Hearing Intervention and Ear Reconstruction — Two Separate Treatment Paths
One thing worth clarifying for families who are thinking about both hearing and ear reconstruction at the same time: these are two separate clinical pathways that do not need to happen in the same sequence or on the same timeline.
Ear reconstruction — rebuilding the outer ear using the child’s own rib cartilage — is focused on the visible structure of the ear. Hearing intervention addresses the function of the middle ear and the pathway to the cochlea. Dr. Bonilla evaluates each child’s anatomy individually and helps families understand how these two goals interact for their specific situation.
Some families prioritize hearing first. Some focus on reconstruction first. Some pursue both in a carefully coordinated sequence. The appropriate sequence depends on each child’s specific anatomy and the family’s priorities — Dr. Bonilla evaluates these individually.
What to Do If Your Child Was Just Diagnosed
If your child was recently diagnosed with microtia, the key points to carry forward are these: The inner ear is almost certainly fine. The hearing nerve is almost certainly intact. There is a clear, well-established approach to both hearing management and reconstruction, and Dr. Bonilla’s team is available to help families understand what applies to their child specifically.
Schedule a hearing evaluation. Reach out to a microtia specialist. Ask every question you have.