Natural Rib Cartilage vs. Medpor/Su‑Por: A Clinical Comparison
The choice between natural rib cartilage and synthetic implant reconstruction is one of the most important decisions families face after a microtia diagnosis. This page presents a comparison of both approaches based on peer-reviewed literature and Dr. Bonilla’s thirty years of clinical experience — including the genuine advantages and disadvantages of each.
The patient’s own living tissue — grows with the child, cannot be rejected, flexes under impact, requires no replacement — ever.
Medpor/Su-Por requires 7–10+ hours of anesthesia — longer than Dr. Bonilla’s entire surgeries combined — and can require revision for fracture or exposure.
Source: Facial Plastic Surgery Clinics of North America — PMID: 29153189

Families researching microtia online will often encounter synthetic implant reconstruction more frequently than rib cartilage, despite rib cartilage being the technique chosen by approximately 91.3%¹ of surgeons in a national ASPS survey (Im et al., Aesthetic Plastic Surgery). Online and social media visibility does not reflect surgeon consensus. Families are encouraged to review peer-reviewed literature and consult with surgeons experienced in both techniques. Dr. Bonilla addresses this directly in his guide on what families are often told — and what experience shows.
Living Tissue vs. Synthetic Material — Why This Difference Matters
The comparison between natural rib cartilage and Medpor/Su-Por (porous polyethylene) is often framed as a debate about surgical stages, chest scars, and recovery times. These are genuine considerations. But they are secondary to the primary question, which is:
What should a reconstructed ear actually be made of?
Rib cartilage is the child’s own living biological tissue. After it is carved into an ear framework and placed beneath the skin, the body does not merely tolerate it — it integrates it. The cartilage chondrocytes remain viable. The framework acquires vascular connections through surrounding tissue. The immune system recognizes it as self. Over time, the ear grows alongside the child’s face because it is, biologically, part of the child.
Medpor/Su-Por is porous high-density polyethylene — a rigid, synthetic plastic. The porosity allows fibrovascular tissue to grow into it, which stabilizes it, but the material itself is and always will be inert and foreign. It does not grow. It does not acquire biological properties. It remains, from the first day of implantation onward, a foreign body within the surrounding tissue.
This distinction is not philosophical — it has direct, concrete clinical consequences that play out over a child’s lifetime. Most of the downstream differences between the two approaches — in complication rates, revision difficulty, activity restrictions, and long-term outcomes — flow directly from this fundamental difference in material nature.
What both approaches share
It is worth being honest about where the approaches converge. Both, in experienced hands, can produce aesthetically detailed ears that provide meaningful psychological benefit to children and families. Both require surgical skill and significant surgical experience to achieve good results. Both have genuine bodies of published outcomes literature. And both represent a serious, committed attempt to restore something important to a child who was born without it.
The disagreement is not about intentions or effort. It is about which approach produces the best outcome across a child’s lifetime — not just in the first year after surgery, but at age 15, 35, and 65.
What happens if revision is needed
With natural rib cartilage reconstruction, the skin and tissue environment is preserved — meaning options remain open for microtia treatment even if the reconstruction requires additional work. Critically, natural cartilage reconstruction should always be performed before any synthetic implant surgery. If a cartilage reconstruction is attempted first and requires further work, the surgeon is still operating in a healthy, unscarred tissue field. If a synthetic implant is placed first and complications arise, the temporoparietal fascia flap has permanently consumed tissue — and its scarring destroys the skin elasticity that natural reconstruction requires. That sequence cannot be reversed. With synthetic implant reconstruction, the temporoparietal fascia flap used to cover the implant is permanently consumed. If the implant needs to be removed or replaced, the tissue required for rib cartilage salvage reconstruction may no longer be available in sufficient quantity — because scarring from the Medpor/Su-Por surgery causes the skin to lose the elasticity required for a successful rib cartilage reconstruction. The first attempt at synthetic implant reconstruction is often effectively the only good attempt.
The Surgical Approach — Both Techniques
Both approaches require incisions at multiple sites. Rib cartilage reconstruction requires two incision sites — the chest for cartilage harvest and the groin for a small skin graft. Synthetic implant reconstruction — Medpor/Su-Por — also requires two incision sites: a scalp incision for the temporoparietal fascia flap and a separate donor site for the skin graft that covers the most visible outer surface of the reconstructed ear.
Natural Rib Cartilage

Rib cartilage harvest incision — a small ¾ inch to 1¼ inch incision is all that is needed to harvest the cartilage. (image)
Rib cartilage donor site — three small pieces of rib are used to match the dimensions of the opposite ear. (illustration)

Rib cartilage post-op — the skin color matches the face because the cartilage was simply placed under a skin pocket with no need for visible skin grafts. The ear has flexibility. (image)
Medpor / Su-Por
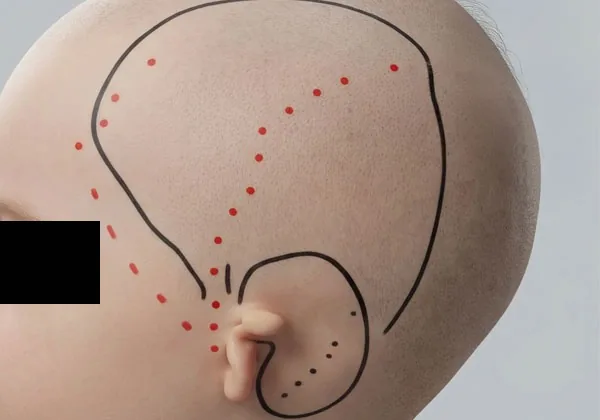
Temporoparietal fascia flap — after shaving the side of the head, a scalp incision harvests a sheet of living tissue used to cover and vascularize the synthetic framework. (rendering)
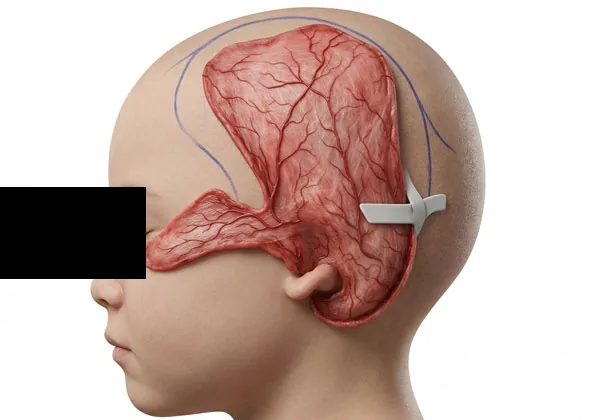
Temporoparietal fascia flap — extensive undermining of the scalp up to near the midline occurs to cover the synthetic plastic implant with a vascular flap. Care is taken to avoid damaging a branch of the facial nerve. (rendering)

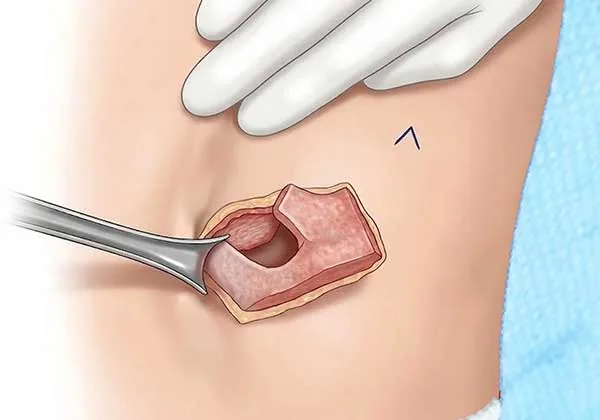
Synthetic plastic implant ear — full-thickness skin grafts are placed to cover the shortage of natural skin over the ear. Skin color varies as the grafts mature. (rendering)
What Families Often Did Not Anticipate Before Synthetic Implant Reconstruction
Families who consult Dr. Bonilla after synthetic implant reconstruction frequently report that certain aspects of the procedure or recovery were not what they had anticipated beforehand. These are the factors most commonly raised.
The porous polyethylene implant remains rigid for the rest of the patient's life. It does not soften or become more natural over time. Discomfort when lying on the reconstructed ear is a commonly reported long-term complaint.
The skin graft placed over the most visible outer surface of the reconstructed ear is taken from a donor site elsewhere on the body. This donor skin may differ in color and thickness from the child's surrounding natural skin — a difference that does not resolve over time.
Because much of the visible ear surface is covered by a skin graft rather than the child's native skin, sensation in the reconstructed ear is typically reduced compared to natural tissue.
Dissection of the temporoparietal fascia flap requires an incision in the scalp area. Hair loss at this site is a documented risk that may be permanent.
Medpor/Su-Por reconstruction requires shaving most of one side of the head and scalp to access the temporoparietal fascia flap. Rib cartilage reconstruction requires shaving approximately 1–2 centimeters only — localized to the immediate surgical area.
The temporoparietal fascia flap dissection is performed in proximity to branches of the facial nerve. Damage to one of these branches is a documented surgical risk.
The weight of the porous polyethylene implant can cause the reconstructed ear to migrate downward over time.
Because porous polyethylene is a rigid material, the reconstructed ear carries a risk of fracture or displacement under significant impact for the rest of the patient's life. This risk does not diminish with healing.
The implant can breach the overlying skin through trauma or gradual pressure over time. A 2025 meta-analysis of 11 studies covering 3,816 patients found that porous polyethylene implants had a framework exposure rate approximately 6.97% higher than autologous rib cartilage reconstruction. Source: Finestone et al., Cleft Palate Craniofac J, 2025. This risk does not resolve with healing — it is a permanent material property.
Synthetic implant reconstruction typically requires 7 to 10+ hours under general anesthesia.
Choosing synthetic implant reconstruction first significantly limits future options. The temporoparietal fascia flap and surrounding tissue are permanently consumed during the procedure. If the result is unsatisfactory or complications develop, the tissue required for rib cartilage salvage reconstruction may no longer be available in sufficient quantity — because scarring from the Medpor/Su-Por surgery causes the skin to lose the elasticity required for a successful rib cartilage reconstruction. This is a documented clinical consequence of the procedure — not a theoretical concern. Families dealing with the aftermath of a poor prior result will find a detailed clinical discussion of options after a poor prior result on the revision surgery page.
A synthetic implant does not grow. The surgeon must estimate the patient's future adult ear size at the time of surgery and implant a fixed framework accordingly. Natural rib cartilage, by contrast, is living tissue with its own circulation — it integrates biologically and grows proportionally with the patient's face for life. A child whose face continues to grow around a fixed synthetic implant may develop a size asymmetry between the reconstructed ear and the natural ear over time.

Hair loss from dissection of the temporoparietal fascia flap after porous synthetic ear implant surgery.

Skin breakdown, exposure of the porous synthetic ear implant and eventual fracture of the implant.

Exposure of the porous synthetic ear implant as well as different skin color from a full-thickness skin graft.
A Side-by-Side Comparison
A structured comparison across the clinical factors most relevant to long-term outcome.
¹ Finestone SA et al., Cleft Palate Craniofac J 2025 — systematic review and meta-analysis of 11 studies covering 3,816 patients: porous polyethylene implants associated with higher framework exposure (6.97% difference), infection (3.18% difference), and redo procedures (4.88% difference) compared to autologous rib cartilage reconstruction.
Complications and Risk Profile
Every surgical approach carries risk. The question is not whether risk exists but what form it takes, how manageable it is, and what happens when it materializes.
On the exposure rate: A 2025 systematic review and meta-analysis of 11 studies covering 3,816 patients found that porous polyethylene implants had higher pooled rates of framework exposure, infection, and redo procedures compared to autologous rib cartilage reconstruction. The framework exposure rate difference was 6.97% (95% CI: 0.07–13.86%). The key concern is not the rate itself but what happens when exposure occurs — the ingrown fibrovascular tissue makes safe removal and revision extremely difficult. View full research summary →
Six Claims About Medpor/Su-Por — Addressed Directly
These are the arguments that come up consistently in favor of Medpor/Su-Por reconstruction. Some have merit. Some are misleading. Each deserves a complete, honest answer.
The advantage is real. Medpor/Su-Por can be performed as early as age 3, and rib cartilage reconstruction typically requires waiting until age 6–9. For families who want to address the ear before kindergarten or early school years, this is a genuine clinical advantage of the Medpor/Su-Por approach.
The context that usually gets omitted: Children under 6 have a limited understanding of what surgery is and why it is happening. Dr. Bonilla’s experience is that children under 6 are often more anxious, less cooperative, and less able to participate meaningfully in the consent and preparation process. Children at age 6 and older have a substantially better experience with the surgical process itself.
More importantly: the 2–3 years of waiting for cartilage surgery does not mean doing nothing. Many families use prosthetic ear covers or hairstyling during this period. The question families should ask themselves is: is gaining 2–3 years worth the long-term trade-offs in complication risk, growth asymmetry, and revision difficulty? For some families, it is. That is a legitimate choice. But the trade-offs should be part of the conversation.
In Dr. Bonilla’s practice, the chest incision averages approximately 1¼ inches — closer to two inches in larger patients. In thinner patients it can be closer to one inch. It is placed low on the lateral chest wall, heals in layers, and becomes a fine, faded scar over the following one to two years. In over 30 years and thousands of procedures, Dr. Bonilla has not seen a single chest wall deformity caused by cartilage harvest.
The claim that cartilage surgery is “more invasive” is also worth examining from the other direction. Medpor/Su-Por surgery requires a temporoparietal fascia flap — scalp tissue is elevated above the ear, pulled down over the implant, and covered with a skin graft. This is an independent surgical procedure with its own risk of hair loss, scalp scarring, and flap-related complications. Whether a chest incision or a scalp flap is “more invasive” is debatable. What is not debatable is that the scalp procedure carries real independent risks that rib harvest does not.
Protrusion is achievable with both techniques. With Medpor/Su-Por, a rigid synthetic implant forms the entire ear structure and is engineered to project outward. Dr. Bonilla’s technique is fundamentally different: the ear itself is built entirely from the child’s own natural rib cartilage — carved by hand, placed as living tissue, growing with the child for life. To maintain projection permanently, Dr. Bonilla designed the Microtia Wedge — a small internal support piece of porous polyethylene positioned entirely behind the cartilage framework, never forming any part of the visible ear structure. The ear is cartilage. The wedge holds the angle. The Microtia Wedge lies flat against the skull in a fully protected position, covered by overlying tissue, with no surface exposure. This technique was developed specifically to avoid harvesting additional rib cartilage, and because of its success it is now being adopted by cartilage surgeons worldwide. This is categorically different from synthetic implant reconstruction, in which the polyethylene framework is the ear — requiring a temporoparietal fascia flap and carrying lifetime exposure and fracture risks. In Dr. Bonilla’s reconstruction, no synthetic material forms, touches, or constitutes any part of the ear.
More importantly, protrusion has a practical ceiling. An ear that protrudes too much looks bulky and unnatural. The goal is an ear that protrudes enough to allow glasses to be worn comfortably — not an ear that maximizes projection. And here is a critical practical point: a highly protruding rigid implant is painful to sleep on. This is one of the most common complaints Dr. Bonilla hears from families seeking second opinions after Medpor/Su-Por surgery — the child cannot comfortably sleep on the implant side. Cartilage, having natural flexibility, does not cause this problem.
This is one of the most persistent misconceptions, and it may reflect genuine differences between surgical practices rather than inherent properties of the technique. In Dr. Bonilla’s practice, every patient receives a small epidural nerve block during surgery while asleep, targeting the rib area specifically. Patients wake up numb from the chest. They go home the following morning with acetaminophen (Tylenol) syrup.
On a 1–10 pain scale, the vast majority of Dr. Bonilla’s patients consistently rate their post-operative pain at 1 or 2. The experience is so mild that staff often have to remind patients to rest rather than try to resume normal activity too quickly.
The claim that cartilage surgery requires hospital stays of a week for pain management is not consistent with modern anesthetic technique. Dr. Bonilla’s patients stay one night for monitoring — not pain control — and are discharged the following morning. The one-night stay reflects Dr. Bonilla’s philosophy that children undergoing lengthy anesthesia should be monitored by nursing staff while parents rest, not that the pain requires prolonged inpatient management.
The cartilage technique has published follow-up data spanning 20–30 years showing stable, well-maintained results into adulthood. The Medpor/Su-Por technique does not have comparable long-term comparative data. Studies that do follow patients over longer periods show higher complication rates, more revision surgeries, and outcomes that diverge from cartilage as time passes — particularly in growth asymmetry and complication accumulation.
This claim also omits the important distinction between “good results in the short term” and “good results across a lifetime.” An ear that looks good at age 5 may not look as good at age 20 if it has not grown with the face. An ear that never had complications may still require surgery at age 30 if the implant extrudes. The time horizon matters enormously.
The most honest answer: We do not yet have equivalent long-term data for Medpor/Su-Por that would allow a rigorous apples-to-apples comparison with 30-year cartilage outcomes. What we do have suggests the long-term trajectory for cartilage is better. Absence of proof is not proof of equivalence.
A Medpor/Su-Por implant ear can be moved up and down on the head during surgery — positioned at different heights. In that sense, “movement” during placement is possible. But what matters functionally is what happens after surgery, in daily life.
Porous polyethylene is a hard plastic. It does not flex with normal movement. It does not yield to pressure the way cartilage does. This is why patients with highly protruding Medpor/Su-Por implants commonly complain of discomfort when lying on the ear — the implant does not give, so the pressure is constant and rigid. A cartilage ear has natural biological flexibility. It gives slightly with pressure and returns to shape, which is far more comfortable and far more durable under impact.
Dr. Bonilla’s Clinical Position
Dr. Bonilla does not use Medpor/Su-Por as the ear reconstruction framework. He does not rotate between techniques based on what a family asks for. The reconstructed ear is always built entirely from the child’s own natural rib cartilage — and has been for 30 years. He does use the Microtia Wedge — a small Su-Por support piece he designed — placed behind the cartilage ear during elevation to maintain projection. It is never visible and forms no part of the ear structure.
This is not a reflexive conservatism or resistance to new techniques. Dr. Bonilla has studied the Medpor/Su-Por literature carefully throughout his career. He has seen the patients who arrive at his practice for second opinions following failed Medpor/Su-Por surgery — some of them seeking revision that is difficult or impossible due to the compromised tissue left behind. He has also read the studies that Medpor/Su-Por proponents cite, and his assessment of the evidence differs from theirs.
His core conviction: There is no manufactured material that replaces living biological tissue. This is not a controversial medical claim — it is basic biology. The question is not whether cartilage is theoretically superior. The question is whether the short-term advantages of Medpor/Su-Por (earlier timing, fewer initial stages, no chest scar) are worth the long-term disadvantages (growth asymmetry, higher complication rates, extremely limited revision options). His answer, after 30 years and thousands of cases, is no.
On the social media problem
Online communities for microtia families can be a valuable source of peer support, but they are not a substitute for direct consultation with surgeons who perform both techniques. Seek information from multiple sources, including peer-reviewed literature, before making a final decision.
On the “best in my hands” argument
Some surgeons who offer Medpor/Su-Por argue that results are best with the technique a surgeon knows most deeply. Dr. Bonilla acknowledges this as a genuine clinical truth — experience with a specific technique does improve outcomes. His point is that this logic, applied rigorously, argues for exclusive specialization rather than against it. The logic of exclusive specialization is that depth of experience with a single technique produces refinement that is only achievable through that kind of focused repetition. That is what 30 years of exclusivity produces.
On families who have already chosen Medpor/Su-Por: Dr. Bonilla does not believe that every Medpor/Su-Por outcome is poor. Many patients have good results, and for families for whom earlier timing was the right decision, that decision may have been correct. He is not here to tell parents they made a mistake. His role, for families still making the decision, is to ensure they have complete information — not selectively presented information.
Dr. Bonilla performs reconstruction between ages 6 and 9 for a reason that goes beyond rib cartilage development. He believes the child should have meaningful input into a permanent decision about their own body. A child who is old enough to understand what surgery involves — to ask questions, express their feelings, and participate in the process — arrives at surgery differently than a child who had no say. The claim that earlier is better because the child will never remember misses this point entirely. Memory is not the standard. Participation is. A 6 to 9 year old child who has been part of the conversation, who understands what is happening and why, recovers differently — and relates to their result differently — than a child who had no input. That distinction matters to Dr. Bonilla. It has always been part of how he practices.
If You or Your Child Have Already Had Medpor/Su-Por Surgery
This page is written primarily for families who are still making their decision. If your child has already had Medpor/Su-Por reconstruction, this information is not intended to cause alarm, regret, or second-guessing. Many patients have good outcomes with Medpor/Su-Por, and outcomes across practices vary significantly based on surgeon experience and technique.
If your child’s reconstruction went well and your child is happy: That is what matters. You made the best decision you could with the information you had, with the surgeon you chose, and the result has been good. No page of clinical comparisons should disturb that.
If you are experiencing complications or dissatisfaction following Medpor/Su-Por surgery — exposure, infection, asymmetry, pain, or result that does not meet your child’s expectations — Dr. Bonilla sees patients in these situations. He will evaluate honestly what revision options exist. The situation is more complex than in a first reconstruction, and he will not promise outcomes he cannot deliver, but he will give you a complete and candid assessment.
If your child has not yet had surgery but another surgeon has recommended Medpor/Su-Por: a consultation with Dr. Bonilla is a second opinion, not a commitment. It is appropriate to hear from a surgeon who exclusively performs cartilage reconstruction before making a final decision.
Questions Every Parent Should Ask Any Microtia Surgeon
These questions apply whether you are consulting with Dr. Bonilla or any other surgeon — cartilage or Medpor/Su-Por. Good surgeons will answer them directly.
The Future of Microtia Reconstruction: Tissue Engineering
The longer-term scientific trajectory of microtia reconstruction is not Medpor/Su-Por versus cartilage — it is tissue engineering. Researchers worldwide are working on growing ear-shaped cartilage frameworks in the laboratory from the patient’s own cells. The goal is an ear that is biologically the patient’s own, like rib cartilage, but without requiring any harvest procedure.
The reason tissue engineering research is focused on cartilage — not synthetic materials — is itself informative. The scientific consensus among researchers is that the ideal outcome is living, autologous biological tissue. Synthetic implants are not the future they are working toward; they are the compromise that current technology requires in some contexts.
Dr. Bonilla watches this research closely. He believes laboratory-grown cartilage represents a genuine advance if and when it becomes clinically available — and that when it does, it will be adopted quickly because it addresses the only meaningful limitation of current cartilage reconstruction: the need for a chest harvest.
Request a Consultation
Dr. Bonilla offers consultations for microtia families worldwide — including telehealth appointments for families who cannot travel. He will review your child’s specific anatomy and grade, discuss candidacy and timing, and answer your questions directly.
To request a consultation, submit your information through our contact form and Dr. Bonilla’s team will be in touch to schedule a virtual appointment.