
World’s Only Exclusive Pediatric Microtia Surgeon For Over 30 Years
Microtia
Dr. Arturo Bonilla
Pediatric Microtia Surgeon - San Antonio, Texas
Microtia is a congenital ear deformity where the outer ear is underdeveloped or absent (anotia). Occurring in approximately 1 in 6,000 to 12,000 births, it often affects the right ear and is frequently accompanied by aural atresia (absence of an ear canal), leading to conductive hearing loss. While the diagnosis can be overwhelming, the inner ear is usually healthy, making successful reconstruction and hearing restoration possible.
Medically reviewed by Arturo Bonilla, MD — August 2026
What is microtia?
The term “microtia” is derived from the Latin words micro (small) and otia (ear). It is a congenital condition that develops during the first trimester of pregnancy. While it can occur as part of a spectrum like Hemifacial Microsomia or Treacher Collins Syndrome, in most cases, it is a random, isolated event.
Microtia occurs in approximately 1 in 6,000 to 12,000 births. It is more common in males and often affects the right ear more than the left.


What Grade I looks like
All recognizable anatomical structures are present: the helix (outer rim), antihelix, tragus, concha, and earlobe. The ear is clearly identifiable as an ear from any normal viewing distance. What distinguishes it is that it is smaller than normal, and one or more structural elements may be underdeveloped or misshapen.
Common features: a helix that does not complete its curve, a shallower concha, a smaller or absent tragus, or an overall ear noticeably smaller than the opposite side. In some cases the differences are subtle; in others the asymmetry is obvious to any observer.
How Grade I affects hearing
Grade I typically causes mild to moderate hearing reduction — less than higher grades because more outer ear structure is present. Many children with Grade I hear well enough for normal speech and language development. However, they still benefit from audiology evaluation and monitoring, as even subtle hearing differences between ears can affect spatial hearing and classroom performance.
Dr. Bonilla's surgical approach for Grade I
Grade I patients rarely require surgery. A slightly smaller but naturally formed ear is almost always preferable to a reconstructed one — and in most Grade I cases the ear retains enough natural structure that reconstruction would offer little meaningful improvement. However hearing evaluation is still essential — an Auditory Brainstem Response test should be performed early to confirm the hearing status on the affected side, as hearing can still be affected even when the outer ear appears nearly normal. Dr. Bonilla monitors Grade I patients carefully over time — tracking hearing, development, and the child’s own perspective as they grow. If any intervention is ever considered it is discussed openly with the family and the child when age appropriate.

What Grade II microtia looks like
Grade II is defined by a partially formed outer ear — some recognizable structures are present, but a significant portion is absent. The most common presentation is an upper or lower portion of the ear that has formed with some identifiable shape, while the rest is absent or vestigial. A small hook-shaped cartilage remnant with a displaced earlobe is also common. The ear canal is typically absent or severely narrowed in Grade II.
How Grade II affects hearing
With the ear canal typically absent, Grade II produces a moderate to moderately severe conductive hearing loss of approximately 45–60 dB. The inner ear is almost always fully functional — this is a blockage problem, not a nerve problem. Bone conduction typically reveals normal inner ear function. A bone-anchored hearing aid (BAHA) is the standard early hearing management strategy.
Dr. Bonilla’s surgical approach for Grade II
Dr. Bonilla completes Grade II reconstruction in one surgery using the child's own rib cartilage.
What Grade III microtia looks like
Grade III is what most people picture when they hear the word microtia. It is by far the most common presentation — approximately 7 in 10 children with microtia have Grade III. The defining feature is a small, irregular cartilage remnant — often described as peanut-shaped, sausage-shaped, or “crumpled.” This remnant is residual cartilage tissue that did not develop into a recognizable ear structure. Below or attached to it is a displaced earlobe — a small tag of skin representing surviving lobule tissue. There is no ear canal.
How Grade III affects hearing
With no ear canal, Grade III produces a moderate-to-severe conductive hearing loss of approximately 40–60 dB on the affected side. But the unaffected ear does most of the work. Most children with unilateral Grade III develop normal speech and language with no intervention — the brain compensates remarkably well. There are real-world impacts though: difficulty in noisy environments, inability to locate the direction of sounds, and listening fatigue. Many families choose a BAHA softband during early childhood; others monitor without a device.
Dr. Bonilla’s Surgical Approach for Grade III
Grade III reconstruction is completed in two stages over approximately two months.
Stage 1: The rib cartilage framework is harvested, hand-sculpted, and placed. The preserved earlobe is rotated into position, the tragus is formed, and the conchal bowl is deepened. Drains maintain close skin-to-cartilage contact during healing.
Stage 2: The ear is elevated from the head to create natural projection. A skin graft placed behind the ear supports the sulcus, and a BAHA implant can be placed concurrently if chosen. The reconstruction is complete.

What Grade IV (anotia) looks like
Anotia is the complete absence of the external ear. There is no peanut-shaped remnant, no earlobe, no cartilage nub — the side of the head is smooth where the ear would be. No ear canal, no external opening of any kind. The skin over the area is intact and completely normal; it simply has no ear on it.
Anotia is rare — approximately 5% of microtia cases. It occurs more often in bilateral microtia (both ears affected) than in unilateral cases, though it can and does present on one side alone.
Surgical Considerations for Grade IV
Parents hearing “there’s nothing there at all” naturally feel more alarmed than parents of Grade III children. Anotia cases, while requiring careful planning, benefit from an undisturbed skin surface that allows precise framework placement without navigating misformed tissue. The reconstructed ear is placed exactly where it belongs, on undisturbed skin.
Because no earlobe tissue exists, the lower part of the framework is shaped as the earlobe during Stage 1. Stage 2 elevates the framework and creates the final projection.
Dr. Bonilla’s surgical approach for Grade IV
Grade IV follows the standard two-stage protocol. In Stage 1, Dr. Bonilla creates and places the complete cartilage framework, including the lower portion that forms the earlobe. In Stage 2, the ear is separated from the head and elevated to its final position.
What It Looks Like
Bilateral microtia means both ears are affected. Each ear may present at a different grade — one ear may be Grade III while the other is Grade II, or both may be the same grade. The condition occurs in approximately 10% of microtia cases and presents unique considerations for both hearing and reconstruction that differ meaningfully from unilateral cases.
Hearing Management
When both ears are affected hearing intervention is not optional — it is essential from the earliest possible age. A bone conduction hearing aid softband should be fitted ideally within the first two months of age. Unlike unilateral microtia where the unaffected ear compensates, bilateral microtia means the child has no natural hearing pathway on either side. Without early intervention speech and language development can be significantly affected. An Auditory Brainstem Response test should be performed as early as possible to confirm inner ear function — which is almost always intact — and to establish the foundation for a hearing plan.
Surgical Approach
For bilateral reconstruction, Dr. Bonilla coordinates both ears across three surgical visits over approximately four months. Visit 1 is Stage 1 on Ear 1. Visit 2 combines Stage 2 on Ear 1 with Stage 1 on Ear 2 under the same anesthesia. Visit 3 is Stage 2 on Ear 2. Each ear has its own rib cartilage harvest, taken from the side of the chest opposite the ear being reconstructed, during that ear’s Stage 1.
What Families Should Know
Bilateral microtia is a more complex presentation but it is one Dr. Bonilla has extensive experience with. Families with bilateral children are encouraged to reach out early — not because surgery is urgent, but because the hearing plan needs to begin immediately and the surgical roadmap benefits from early planning. Many children with bilateral microtia go on to live full active lives with natural reconstructed ears and well-supported hearing.
Your Next Steps
Understanding the grade is the beginning of the process, not the end. These are the most useful next resources for families who just received a diagnosis.
Causes & Risk Factors?
Parents often ask, “Did I cause this?” The answer is no. Current research suggests that microtia is largely a random occurrence caused by a temporary disruption of blood flow (possibly via the stapedial artery) during fetal development. It is rarely genetic; the risk of passing it to future children is approximately 5%. It is not caused by the mother’s diet, stress, or activities during pregnancy. Click our Causes & Risks page for more detailed information.
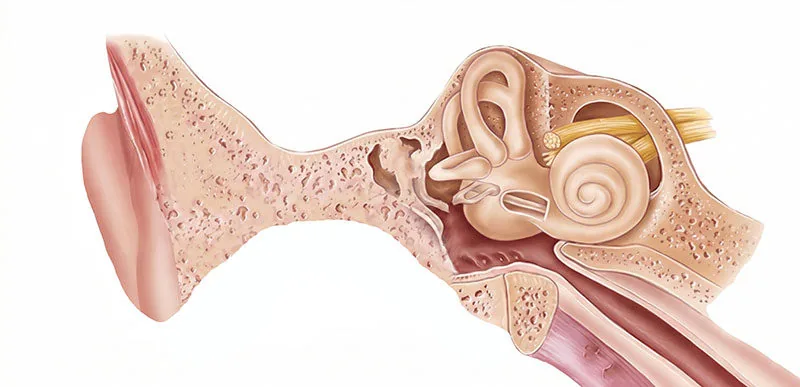
Aural Atresia & Hearing Loss
Microtia mainly affects the outer ear, but it is often linked to Aural Atresia, the absence of an ear canal. This results in “conductive hearing loss,” where sound cannot reach the middle ear. However, the inner ear (cochlea) and hearing nerve are usually perfectly normal.
* The Solution: Dr. Bonilla coordinates closely with audiologists to manage hearing. Treatment options such as BAHA (Bone-anchored Hearing Aids), softband for infants or surgical canal reconstruction (Atresiaplasty) is explained in our Hearing Options page.
Pediatric Ear Reconstruction: The Rib Cartilage Standard
Dr. Arturo Bonilla utilizes the autologous rib cartilage technique, widely considered the “Gold Standard” for pediatric ear reconstruction. Unlike synthetic plastic implants (Medpor), which carry lifelong risks of infection, extrusion, and fracture, the living rib cartilage:
- Grows with the child: Ensuring the new ear remains symmetrical as the patient ages.
- Heals naturally: Since it is the patient’s own tissue, there is no risk of rejection.
- Withstands trauma: Children can play sports and lead active lives without fear of damaging a plastic implant.

Frequently Asked Questions
Is microtia surgery cosmetic?
No. Microtia reconstruction is reconstructive surgery intended to correct a congenital deformity and improve quality of life. Therefore, it is typically covered by insurance plans.
At what age should microtia surgery be performed?
Dr. Bonilla recommends beginning reconstruction between 6 and 9 years of age. At this time, the child has sufficient rib cartilage to craft a detailed ear framework, and the “normal” ear has reached near-adult size, allowing for perfect symmetry.
Can microtia be detected on an ultrasound?
Microtia is often missed on prenatal ultrasounds because technicians focus on vital organs like the heart and kidneys. Many parents only discover the condition at birth.
Is microtia hereditary?
Microtia is usually not inherited, but in rare cases, there may be a genetic link or family history of ear anomalies. It is recommended to seek a Geneticist specialist for a complete patient and family assessment for future risks.
Can microtia occur with other conditions?
Yes, microtia may be associated with conditions like hemifacial microsomia, Treacher-Collins syndrome and Goldenhar syndrome. However, many children with microtia are otherwise healthy.
What tests are needed after birth?
While the newborn with microtia is still in the hospital, a newborn hearing screening is always performed. Usually the baby with microtia will pass on the normal side and fail on the microtia side. This does not mean the patient is deaf. It just means that there is some type of hearing loss that needs to be further evaluated. Once the patient is discharged from the hospital, an auditory brainstem response test (ABR) is recommended to evaluate in more detail the function of the auditory or hearing nerve. Most patients have a normal hearing nerve, even on the side of the microtia. This means that sound is just muffled on that side without deafness. As stated above, a CT scan of the ears is performed at a later age (usually 4–5 years of age) to evaluate the anatomy of the outer, middle and inner ears to determine if the child is a possible candidate for opening up the ear canal. An audiological evaluation is also very important. A full ENT evaluation is also recommended.
How is microtia diagnosed?
Microtia is usually easily diagnosed at birth. When the microtia is very minor (Grade 1 microtia), it may be more difficult to diagnose. Imaging studies like a CT scan may be used to evaluate the inner ear structures and determine candidacy for hearing improvement via bone-conduction hearing aids or surgery at a later age.
When should my child see a microtia specialist?
Dr. Bonilla recommends consulting a microtia specialist as early as the day of birth to help parents understand the condition and outline a plan for hearing and reconstructive care. During this time, there is much stress from the parents and this is a perfect time to let the parents know that everything will be ok and that their child is not deaf. This is also a good time to give the parents a general plan for the management of the microtia as well as management of the hearing.
Dr. Bonilla has been treating pediatric microtia patients for over 30 years.
What are the treatment options for microtia?
The most common treatment used by 99% of surgeons worldwide is the rib cartilage option because it is natural, grows with the patient, and avoids risk of fracture or exposure. Other options include synthetic plastic polyethylene Medpor / Supor surgery. A prosthetic is typically a last resort option. Hearing restoration may involve bone conduction hearing aids or ear canal surgery, depending on the anatomy. Microtia Treatment Options →
Which 3D reconstruction method is best?
The best method depends on your child’s anatomy, medical history, and your surgeon’s expertise. Rib cartilage surgery (the most common and gold-standard) is natural and long-lasting, while Medpor / Supor offers earlier reconstruction but with different risks such as fracture or exposure of the new ear for the rest of the patient’s life. Surgeon experience is absolutely critical using the above techniques in order to avoid a lifetime of dealing with a poor aesthetic result.
Can children with microtia hear?
Children with microtia usually have moderate to severe conductive hearing loss, especially if they also have aural atresia. However, their inner ear (cochlea) function is usually normal, and hearing can be improved with hearing devices or surgery.
What hearing devices can help?
Bone conduction devices such as a BAHA softband can immediately improve the hearing via bone-conduction on the skull. Later, the more invasive surgical hearing options are available like the bone anchored hearing aid systems by Cochlear, Oticon, Med-El, usually during the microtia reconstruction. Depending on the result of the CT scan of the ears and on the experience of the ear canal surgeon, the ear canal may also be opened (atresiaplasty).
Can ear canal surgery restore hearing?
In some children with favorable anatomy, atresia repair surgery can create a functioning ear canal and significantly improve hearing. A CT scan helps determine if this is a good option. It is crucial to be evaluated by a very experienced ear canal surgeon in order to avoid damage to the facial nerve, and to decrease the risks of ear canal scarring, etc…
Is microtia associated with psychological effects?
It is important to inform the parents of children with microtia that their lives can be perfectly normal, with or without any type of surgical intervention. Parental confidence is crucial. Dr. Bonilla always gives parents the first option of “doing no surgery at all”. It is common to be pressured to operate on all of these children with microtia, but it should be a decision of the patient as well.
It is not uncommon to receive bullying at school during school age, causing the children to lose self confidence. With early family support and positive reinforcement, the children will do very well and live normal lives without restrictions. Reconstructive surgery with a good result can also improve self-esteem.
How do I support my child emotionally or psychologically?
Encourage open conversations, connect with support groups, and consult with child psychologists or counselors if needed. Highlight your child’s strengths and talents beyond their appearance. It is important to see the “parent’s guide to a child with microtia.”
Can children with microtia attend school and live normal lives?
Absolutely. With proper hearing support and care, children with microtia can thrive academically, socially, and physically like any other child.
ONE-STAGE MICROTIA RECONSTRUCTION Grade 2 Microtia
ADVANTAGES OF THE NATURAL CARTILAGE TECHNIQUE
>94% of world microtia surgeons prefer this technique
Made of cartilage like the natural ear (not plastic)
no chance of fracture nor rejection like Medpor/Plastic ears
Will grow with the patient because it is natural
Dr. Bonilla’s Microtia Surgical Treatment Using the Natural Cartilage Rib Technique
The cartilage technique is the most accepted microtia treatment worldwide using 3D sculpting. Dr. Bonilla has adopted and advanced this method because an ear made of “hard plastic” material for life cannot truly replace the living tissue in natural cartilage. While surgery may not be a medical necessity in some children, Dr. Bonilla strongly believes his surgical microtia treatment can build critical self-confidence in children through ear reconstruction. In comparison to other surgical options, there are many significant benefits to both using the cartilage and the cartilage surgery itself.
The surgery is completed in one or two stages depending on the grade of microtia:
Grade 2 microtia reconstruction is completed in one surgery. The complete ear structure is built from the child's own living rib cartilage, and no additional reconstruction stage is needed.
All other grades requiring full reconstruction are completed in two stages over approximately two months. Stage 1 creates the complete ear structure — framework, earlobe, tragus, and concha. Stage 2 elevates the ear and can include BAHA placement when chosen.
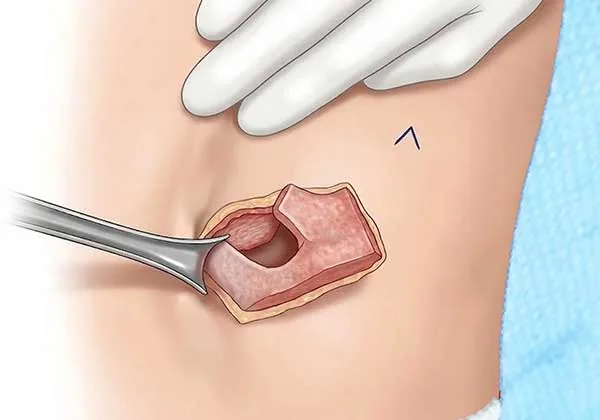
Cartilage Transfer
Dr. Bonilla skillfully transfers cartilage from the child’s rib and uses it to build a proper ear shape. The earlobe and bowl, are created, rotated, and properly positioned.
Various parts of the ear, such as the earlobe and bowl, are created, rotated, and properly positioned.

Enhanced Elevation
Finally, Dr. Bonilla adjusts the ear so that it has separation from the head. A bone-conduction hearing aid can be implanted.
Dr. Bonilla: Microtia Expert & World-Renowned Pioneer
World’s Only Exclusive Pediatric Microtia Surgeon
For microtia patients, nothing replaces the ear like our own living cartilage. Dr. Bonilla exclusively uses this technique in his pediatric microtia patients.
Dr. Arturo Bonilla, with 30 years of experience, has developed techniques that achieve excellent outcomes for children with microtia and atresia.

Letters From Dr. Bonilla’s Patients
Reading the letters written by our children with microtia makes our team feel appreciated and grateful. These letters are so heartwarming and fun to read, we save all of them. We are honored to care for so many children with microtia and atresia worldwide from our San Antonio pediatric microtia surgery office.
How Dr. Bonilla Sets Himself Apart
Extensive Experience
Dr. Bonilla’s career as a pediatric microtia surgeon and fellowship-trained pediatric ENT surgeon has cemented his expertise in both the repair of the microtia as well as the associated hearing loss, allowing him to perform both surgeries simultaneously.
Singular Focus
A typical plastic surgeon performs facelifts, breast augmentations, tummy tucks, and more. Dr. Bonilla only performs microtia surgery using rib cartilage. His singular focus has allowed him to hone his skill to the absolute highest level.
Special Techniques
As part of his constant effort to provide the best treatment for his patients, Dr. Bonilla has developed numerous special techniques including the world’s first successful implantation of a 3D-printed ear made of the patient’s own cartilage.
Lifetime Patient Bonds
Dr. Bonilla exclusively treats children and has a true passion for helping them become their best selves. He treats patients and their loved ones like family, creating lifetime patient bonds with those he helps.
Renowned Expertise
Microtia conferences across the nation have featured Dr. Bonilla as a lecturer. Even the largest microtia and atresia conferences in the country have invited Dr. Bonilla to present as the only cartilage surgeon on the program.
Service and Education
Community service and educating families are critical parts of Dr. Bonilla’s mission. Some patients have gained so much confidence and self-esteem through successful treatment that they become volunteer speakers.
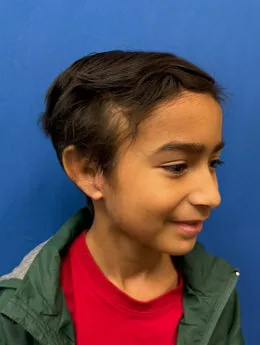
The Life of Microtia Patients
Dr. Bonilla Shows That Microtia Patients May Lead A Normal Life
The pure joy our patients show after successful microtia surgery always puts smiles on our faces. See the children who have undergone Dr. Bonilla’s microtia treatment using the natural cartilage technique and view their ear reconstruction results.

International Pediatric Microtia Clinic!
Caring For Patients Worldwide
As your child’s surgeon, Dr. Bonilla will use small pieces of rib cartilage to perform his advanced microtia repair technique. Ear reconstruction with rib cartilage provides a natural look, feel, and bend for your child’s ear.

Dr. Bonilla’s Passion Has Always Been Helping Children With Microtia!
Dr. Bonilla’s advanced technology and techniques are why so many parents pick him for their children’s life-changing treatment. His natural rib cartilage method, in comparison to the plastic polyethylene alternative, requires shorter surgery times, less anesthesia, and will not break since it uses living tissue. Other examples of Dr. Bonilla’s innovative methods include contact laser technology, which minimizes discomfort.
We know that parents may feel undue guilt when their child has microtia. This diagnosis is by no means your fault, and you can feel comfort in knowing that we can help. In addition to our technological advancements aiding us in providing elite care, they also help keep costs down. At the Microtia – Congenital Ear Deformity Institute, we can make arrangements with most insurance companies to make your child’s treatment as affordable as possible. For compassionate, world-class care from a physician who prioritizes you and your child’s well-being at all times, call or contact us today.

Dr. Bonilla Has 30 Years of Experience as an Exclusive Pediatric Microtia Surgeon
Dr. Bonilla has dedicated his entire career of over 30 years to exclusively taking care of thousands of children born with microtia and atresia. His unique surgical techniques and caring approach have led to global recognition as the leading pediatric microtia surgeon who utilizes children’s own natural rib cartilage.
Your Child May Qualify for Life-Changing Microtia Surgery
During a consultation with Dr. Bonilla, he will examine your child’s ear and determine if they’re a candidate for microtia surgery at our San Antonio office. If they are, our doctor will provide you with thorough pre- and post-operative instructions. If you are traveling a great distance to our San Antonio office, we can help make hotel arrangements for you. Call us if you have questions.
Families from around the globe come to San Antonio to seek treatment with Dr. Bonilla and his advanced natural cartilage techniques.
Major Media Recognition
Dr. Bonilla’s work has been featured by many globally recognized outlets, including CNN, Fox News, CBS, ABC, NBC, Univision, and Telemundo. This is just one of the many stories highlighting his outstanding microtia treatment.
Dr. Bonilla is the only exclusive pediatric microtia surgeon in the world. He has nearly 3 decades of experience having completed thousands of microtia surgeries in children worldwide.
He is an expert in revising failed Medpor and other synthetic plastic ears as well as other failed cartilage reconstructions.

Microtia – Congenital Ear Institute
Dr. Arturo Bonilla
Microtia Congenital Ear Institute is led by Dr. Bonilla, the world's only exclusively pediatric microtia surgeon. Dr. Bonilla has been recognized as one of the leading pediatric microtia surgeons, performing thousands of surgeries for children all over the world. His affiliations include: American Medical Association | American Academy of Otolaryngology
You can contact our office online or by calling (210) 477-3277.
San Antonio Office
9502 Huebner Rd
Ste 301
San Antonio, TX 78240
*Disclaimer: results are not guaranteed, may not be permanent, and can vary per individual. Some images are of models, not actual patients.