Microtia — What It Is, What Causes It, and What Comes Next
If your child was just diagnosed, this guide explains what microtia is, how it affects hearing, the four grades, common causes, and the main microtia treatment options families should understand.
This guide is part of Dr. Bonilla's Microtia Center at Microtia.net, the main resource for families seeking expert microtia reconstruction and treatment.
Microtia is a congenital condition in which the external ear does not fully develop. It can range from a slightly smaller ear to a more complete absence of the ear structure, and it is often associated with hearing differences on the affected side.
If you've just heard this word for the first time, take a breath. Microtia is a congenital deformity of the outer ear, present at birth, that often affects hearing on the same side — and it is treatable. Most children who receive this diagnosis go on to live full, normal lives — many with a reconstructed ear that allows them to move through childhood without the condition defining them.

On Parental Cause
The first thing many parents feel after a microtia diagnosis is guilt. We want to say clearly and immediately: nothing you did or didn't do during pregnancy caused this. Microtia occurs in the first trimester, when the ear is developing from the same tissue as the jaw. The exact cause is not known. It is not genetic in the vast majority of cases. It is not caused by any food, medication, activity, or circumstance that you controlled.
The second thing we want to say: Children who undergo reconstruction and hearing support typically reach developmental milestones normally and live fully without the condition defining them. Most children with microtia achieve successful hearing support and, when they choose reconstruction, a natural-looking permanent ear.
What Is Microtia?
A clear, accurate explanation of the condition — what it is, what it isn't, and why early understanding matters.
The definition
Microtia is a congenital deformity in which the outer ear (the auricle, or pinna) does not fully develop during the first trimester of pregnancy. The word comes from the Latin micro (small) and otia (ear). The condition ranges in severity from a slightly small but otherwise normal-looking ear to the complete absence of an external ear — a condition called anotia.
Microtia affects only the outer ear structure. The inner ear — where the hearing nerve and cochlea are located — is almost always perfectly normal in children with microtia. This is one of the most important and reassuring facts families can know: the hearing system is intact. The challenge is that sound cannot reach it efficiently because the outer ear and often the ear canal didn't fully form.
Unilateral vs. bilateral
Microtia occurs on one side of the head (unilateral) in approximately 90% of cases, and on both sides (bilateral) in roughly 10%. When it occurs on one side only, the right ear is affected more commonly than the left. Unilateral microtia means the child has one normal ear providing full hearing on that side. Bilateral microtia requires earlier and more urgent hearing intervention, since both ears are affected.
What microtia is not
Microtia is not a brain condition. It is not associated with intellectual disability. It is not typically hereditary. It does not affect the child's development, cognition, personality, or health in any way beyond hearing and the appearance of the external ear. Children with microtia are typically healthy, active, and developmentally normal in every other respect.
- Luquetti DV, Leoncini E, Mastroiacovo P. Microtia-anotia: a global review of prevalence rates. Birth Defects Res A Clin Mol Teratol. 2011;91(9):813–822. PubMed →
- Bonilla AR, Tobias AM. Pediatric Microtia Reconstruction With Autologous Rib Cartilage. Plast Reconstr Surg Glob Open. 2018;6(4):e1708. PubMed →
- Luquetti DV, Heike CL, Hing AV, et al. Microtia: epidemiology and genetics. Am J Med Genet A. 2012;158A(1):124–139. PubMed →
The just-diagnosed page is written specifically for parents in those first hours and days — with what actually matters right now, and what can wait.
The Four Grades of Microtia
Microtia is classified by severity on a scale from Grade 1 to Grade 4 (anotia). The grade affects both the surgical approach and, in some cases, the hearing management plan. Most children treated by Dr. Bonilla have Grade 3 microtia, which is the most common form.




How Common Is Microtia, and What Causes It?
Understanding the epidemiology of microtia helps families realize they are not alone — and understanding the microtia causes and risk factors (or lack thereof) helps parents let go of guilt they were never owed. Families looking for a broader starting point can visit our main microtia treatment center for a full overview of Dr. Bonilla's practice.
How common is microtia?
Microtia occurs in approximately 1 in 6,000 to 12,000 births globally, which means it is rare in absolute terms but far from unknown. In the United States alone, several hundred children are born with microtia every year. Worldwide, that number is in the thousands annually.
There are meaningful variations in frequency by population. The condition is more common among boys than girls, and more common on the right side than the left. Certain populations have higher rates of occurrence — including Native American populations and some East Asian populations, particularly in Japan. Ecuador has one of the highest incidence rates in the world. The reasons for these population differences are not fully understood.
The rarity of microtia is also part of why specialized care matters so much: most surgeons — even plastic surgeons and ENTs — encounter it rarely in a general practice. The families who seek out Dr. Bonilla do so precisely because his practice is built around the condition and nothing else.
What causes microtia?
The honest answer is: we don't fully know. Microtia develops during the first trimester, when the ear is forming from tissue structures called the first and second pharyngeal arches. The leading theory is that reduced blood supply to these structures during this critical developmental window disrupts normal ear formation — but why this happens in some pregnancies and not others is not clearly established.
Other factors that have been studied include certain medications taken during pregnancy (particularly some blood pressure medications and some acne treatments used early in pregnancy), viral infections during the first trimester, and environmental exposures — but none of these have been proven as definitive causes, and in most cases of microtia, none of these factors are present at all.
Microtia is not a genetic condition in the vast majority of cases. Parents who have one child with microtia have a very slightly elevated (but still very low) statistical risk with subsequent pregnancies, but in most families, the occurrence is isolated and not inherited. No genetic test currently predicts microtia.
A direct word about parental guilt:
If you are a parent sitting with this diagnosis and wondering what you did wrong — please stop. You did nothing wrong. This has been researched extensively. There is no proven controllable cause. There is no thing you ate, no activity you did or didn't do, no decision you made that caused your child's ear to develop this way. Doctors who have spent careers studying microtia say this clearly and consistently. We say it too, clearly and without reservation.
Hearing, the Ear Canal, and Aural Atresia
The hearing aspects of microtia are often the most confusing — and the most urgent. Understanding them clearly helps families take the right steps at the right time.
The most important thing to understand about hearing in microtia
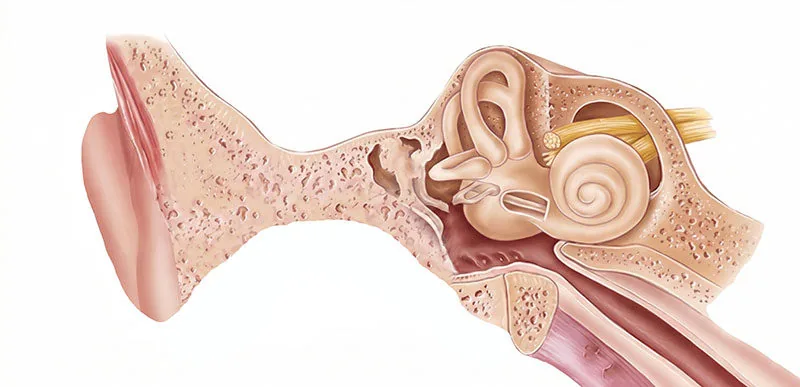
The human hearing system has two major components: the outer and middle ear (which collect and amplify sound and direct it inward) and the inner ear (where the cochlea and hearing nerve convert sound vibrations into signals the brain can interpret). Microtia affects the outer ear. The inner ear — the cochlea and hearing nerve — is almost always completely normal in children with microtia.
What is aural atresia?
Aural atresia is the absence or severe narrowing of the ear canal. Because the ear canal is responsible for directing sound from the outside world to the eardrum and middle ear bones, its absence produces significant hearing loss — typically 40 to 60 decibels of conductive hearing loss on the affected side. To put this in context: normal conversational speech is around 60 dB. A child with atresia who is not wearing a hearing device may struggle to hear a conversation clearly on that side. For a deeper look at how these structures interact, see the guide to ear anatomy and aural atresia.
Aural atresia accompanies microtia in the majority of cases — particularly in Grade 3 and Grade 4. In Grade 1 and some Grade 2 cases, an ear canal may be present, even if narrow. Your child's audiologist and Dr. Bonilla will evaluate whether the canal is present and functional.
The early hearing management window
Because the inner ear is normal, hearing can be effectively delivered by bypassing the absent outer ear entirely — using a bone conduction hearing device. Sound is transmitted through the skull directly to the inner ear through vibration, completely bypassing the absent ear canal. For infants and young children, a soft band device worn on the head delivers this without surgery.
This is not a permanent solution — it is a bridge. But it is an important bridge. The first three years of life are the most critical period for language development, and ensuring a child has adequate access to sound during this window has measurable, lasting benefits for speech, language, and cognitive development.
Early referral to a pediatric audiologist is one of the most time-sensitive actions after a microtia diagnosis. Not because surgery is needed immediately — it isn't — but because hearing management can and should begin very early.
The role of atresiaplasty
Atresiaplasty is a surgical procedure to open the ear canal in children who don't have one — or to widen one that is severely narrow. Not every microtia patient is a candidate; candidacy depends on the anatomy of the middle ear as evaluated by CT scan and scored on the Jahrsdoerfer scale (a grading system for middle ear anatomy). Dr. Bonilla refers patients who are eligible candidates for atresiaplasty to neurotologist specialists for further evaluation and surgical management, coordinating the sequencing carefully so that canal surgery does not compromise the ear reconstruction. For patients who are not atresiaplasty candidates or who elect not to pursue canal reconstruction, Dr. Bonilla performs bone-anchored hearing implant surgery concurrently with ear reconstruction — eliminating the need for a separate surgical procedure and additional anesthesia.
Bilateral Microtia — When Both Ears Are Affected
Approximately 10% of microtia cases affect both ears. Bilateral microtia requires a more urgent hearing management timeline and involves different considerations for surgical planning.
A child with unilateral microtia has one normal ear that provides full hearing on that side. While there are legitimate reasons to support hearing on the affected side — spatial hearing, classroom performance, reducing listening fatigue — the child is never in a situation where they have no functional hearing access at all.
A child with bilateral microtia is in a fundamentally different situation. With both ear canals absent, the child has no natural pathway for airborne sound to reach the inner ears. Without intervention, they face significant hearing loss bilaterally — which has serious implications for language acquisition, speech development, and educational outcomes if not addressed early.
The solution for bilateral microtia is bone conduction amplification, started as early as possible after birth — ideally within the first few weeks of life. A softband bone conduction device (such as a BAHA softband) is non-surgical and can be worn by newborns. It transmits sound through the skull to both inner ears, bypassing the absent canals entirely.
Families with bilateral microtia children should:
- Arrange ABR hearing testing within the first weeks of life
- Get a pediatric audiology referral as soon as possible — ideally before discharge from the birth hospital
- Pursue bone conduction device fitting within 4–8 weeks of birth
- Enroll in Early Intervention services (0–3) which provide speech-language support
- Establish care with Dr. Bonilla to begin the surgical planning process, even though reconstruction itself won't happen for several years
Surgical reconstruction for bilateral microtia follows the same rib cartilage technique as unilateral cases — Dr. Bonilla uses a coordinated staging approach — combining stages across both ears after the first surgical visit to minimize total anesthesia events. Depending on grade, bilateral reconstruction is typically completed in two to four total surgical visits, with the full process taking one to six months.
If you want to understand what a child with bilateral microtia and atresia experiences before receiving a bone conduction device — there is a simple way to feel it yourself.
The inner ear is perfectly fine — the nerve is intact and healthy. The sound simply cannot reach it through the blocked canal. Bone conduction bypasses this entirely by transmitting vibration directly through the skull to the inner ear, restoring clear, full-frequency sound access.
Treatment Options
There are several approaches to treating the outer ear appearance, and several options for addressing hearing loss. Not every option is right for every child — and Dr. Bonilla will help families understand which path makes the most sense for their specific situation. Dr. Bonilla’s thinking on how these decisions are made is covered in depth on the microtia surgery guide. For families who have already had a reconstruction that did not go as hoped, guidance on revision options is also available.
For the outer ear (appearance)
The typical treatment timeline
Recommended First Steps
You don't have to know everything today. But there are a small number of genuinely time-sensitive actions that matter early — and a larger set that can wait. Here's how to think about it.
The most common mistake families make after a microtia diagnosis is either doing too much too fast — overwhelming themselves with research and decisions that don't need to be made yet — or waiting too long to take the steps that genuinely matter in the early months.
The honest summary: surgical reconstruction does not need to happen right away (it can't — the child needs to grow first). But hearing management is time-sensitive, especially in the first three years of life when the brain is most actively laying down language and auditory processing pathways.
Dr. Bonilla's team will guide you through every step of this process. The priority at this stage is hearing assessment and, when relevant, device fitting. Surgical reconstruction does not need to be decided now. When you are ready to understand the full picture, Dr. Bonilla has written a detailed guide on what to know before microtia surgery. Families who would like to review Dr. Bonilla’s clinical background and three decades of exclusive practice can visit the about Dr. Bonilla page.
All of these resources are part of Microtia.net, Dr. Bonilla's dedicated center for microtia families.
Dr. Bonilla has treated thousands of pediatric microtia patients across all four grades — exclusively, for 30 years. A consultation is an opportunity to ask every question you have, understand your child's specific situation, and leave with a clear, personalized plan.